
For months now, we have been bombarded by images of Italians and Spaniards in lockdown expressing solidarity from their balconies, of Jacinda Ardern speaking to New Zealanders from her home, of migrants workers being offered food and shelter in the Indian state of Kerala, of South Korean quarantine kits comprising masks, food and water and much more. Understandably, public interest so far has focused on the most visible aspects of the pandemic response. By looking at empty streets and the number of people wearing masks it was easy to draw comparisons between different countries. And yet, there is another dimension which is just as crucial, but not as tangible – the timeliness of a country’s policy response to the Covid-19 emergency is an even stronger predictor of whether a country has succeeded in preventing death and suffering than the stringency of such measures. This was evident to epidemiologists who are familiar with the exponential way epidemics such as Covid-19 spread; but less so to the general public and policy-makers around the world. In this article, we aim to redress the imbalance of attention between timeliness and stringency.
The key question to be asked then is what made some countries quicker than others in taking measures against the spread of Covid-19. What explains the “success stories” across Hong Kong, Taiwan, South Korea, Thailand, and Singapore? What caused the surprisingly high infection and death rates in the UK, US, Italy, France, and Spain? Scholars of comparative politics have attempted to explain this variation using a set of traditional structural variables: regime type, state capacity, type of leadership, and social buy-in. Some even attribute the successes to an Asian culture that values the community more than individuals. However, these predictors don’t perform well in predicting adequate government response in the Covid-19 crisis. The line between success and failure is not one between authoritarianism and democracy, one between sturdy and weak institutions, or one between communal or individualistic cultures. These variables fail to account for many striking cases in this pandemic: Singapore, as a somewhat authoritarian state, didn’t seem to suffer from the information strain that was supposed to hinder its prompt response; free national health systems in the UK and Italy didn’t prevent some of their hospitals from reaching capacity only a few days into the emergency; Japan, the only country that has yet to enforce any social distancing measures, has kept the virus under control; and Germany, whose population has shown low tolerance for social isolation, seems to be winning its battle against Covid-19.
In the search for a satisfactory explanation as to why some democratic states with strong capacity failed to cope with challenges posed by the Covid-19 crisis, scholars have to depart from conventional variables and consider the role of behavioral and psychological variables – how do the elite and the public perceive such a threat at its emergence and as it develops. Even with the lack of long-range planning and investment, governments’ short-range response could change the trajectory of epidemics. As soon as the novel coronavirus was identified, governments had the option to conduct a quick but comprehensive review of national Personal Protective Equipment (PPE) requirements. Learning from the experience of other countries, some governments put in place a comprehensive testing-manufacturing capability and implemented testing and contact tracing while the number of cases was still low. These short-range behavioral responses determine whether a country could contain the virus wherever it cropped up.
Previous experience is key in driving a timely policy response: at the governmental level, it reduces the uncertainty associated with the choice among several policy options, speeding up the policy-making process. From the public perspective, it heightens the alertness of individuals and promotes higher levels of compliance with precautionary behaviors. In addition, it also increases public demand for policies that prioritize public health over economic and social concerns, thus further legitimating the government’s swift response. Experience of outbreaks of SARS-Cov in 2003 and MERS-Cov in 2015 provides cognitive short cuts and enables a timely response. The key role of previous exposure in shaping a country’s performance in the present emergency is at the same time a humbling lesson and a reason for hope that when similar challenges arise in the future policymakers around the world will be able to respond in a timely fashion.
Debunking the Stringency Myth
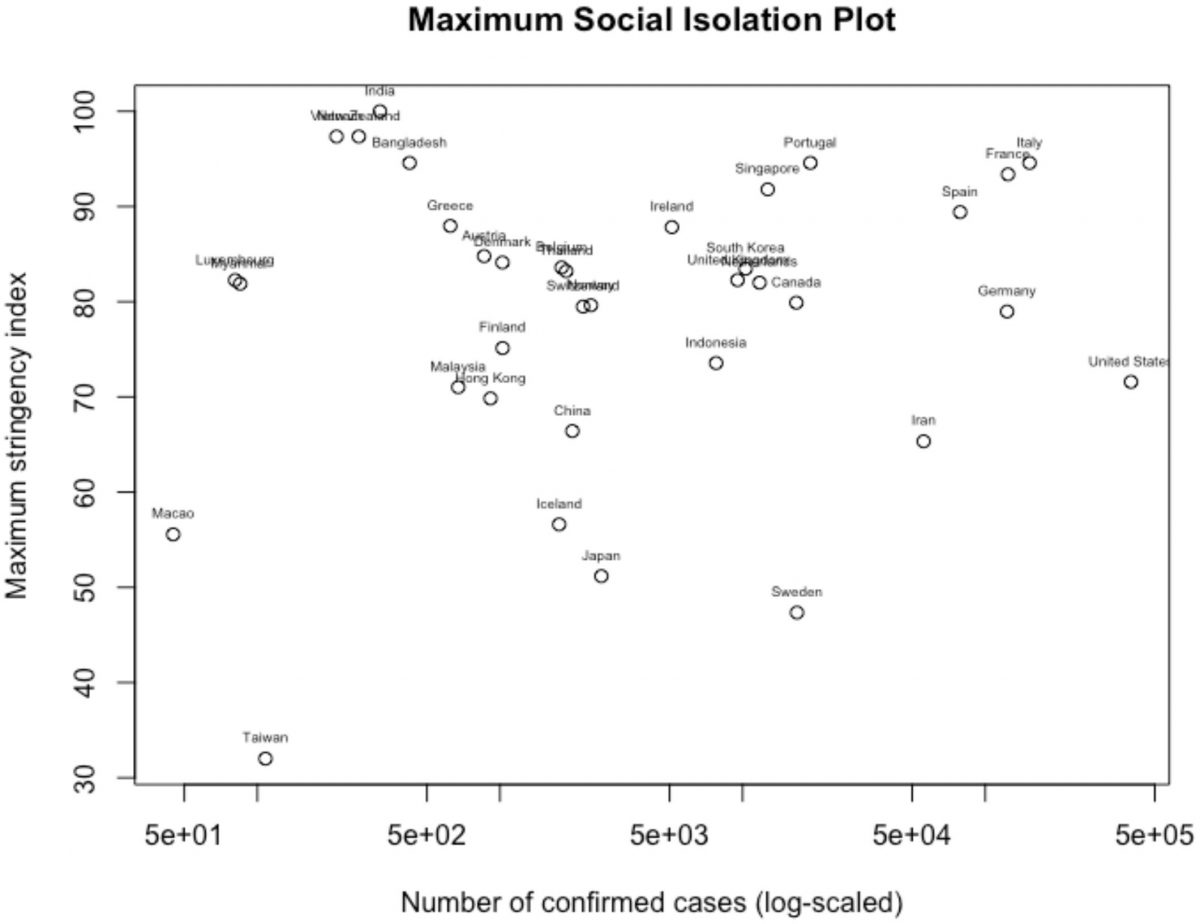
It seems to be a popular belief that countries and regions including Hong Kong, Taiwan, Singapore, South Korea, and Thailand succeeded in containing the spread by enforcing stringent social isolation at high costs in disrupting their socio-economic activities. However, figure 1 shows otherwise. Using the Oxford Coronavirus Government Response Tracker, we plot the maximum stringency level that governments enforced in social isolation during the Covid-19 crisis. Among all the countries considered, Taiwan had the least stringent social isolation even at the peak of infections, while Hong Kong, Macao, South Korea, Thailand, and Singapore all differ significantly in the maximum level of stringency reached with their social distancing measures. Contrary to the popular belief, lockdown in Taiwan, Macao, and Hong Kong were not as stringent as those in most European and North American countries at their climax. Thus, maximum stringency alone – or how costly a lockdown is – does not predict a successful performance at combating Covid-19.
Figure 1. Maximum stringency in social isolation
The Covid-19 virus spreads almost exponentially, which makes it hard to contain in today’s globalized and tightly connected society. Over the last few months, we have seen how rapidly it is transmitted and how hard and costly it is to sever social interactions, once the virus starts spreading locally. Even when a stringent policy of social isolation is implemented, there is a lag between the moment the policy is introduced and the time at which the spread is effectively contained. Better policy timing, therefore, seems to be the key to containment. “Prevention is better than the cure” is a mantra that is often repeated by healthcare workers and scientists alike. With the Covid-19 pandemic, its implications have never been more real. Epidemiologists know very well that the crucial moment for the successful containment of an epidemic is at its early phases, when it remains a ‘potential’ pandemic and not already a given fact. At this pivotal stage, the most effective measures are not necessarily the most stringent, but rather those that give the most precise picture of the state of affairs: identifying the virus and estimating its infectivity rate, and implementing contact tracing and population screening measures are all examples of an early-stage, precautionary approach. Whether these measures are successfully implemented depends on the timing of the government, but also on the compliance of the public at a time when the virus has not caused too much damage, yet.
Risk Perception and Behavioral Response in the Covid-19 Outbreak
It is no rare case that simple structural differences do not account for the variations observed in this global crisis. In the context of the Covid-19 pandemic, comparative politics scholars would argue that democracy facilitates better information flow, hence leaders of the democratic governments are in a better position to make swift and judicious decisions when a pandemic breaks out. Strong institutional capacity enables this decision to be implemented throughout, and it can be better enforced in democracies because people show higher levels of trust in institutions. The 2019 Global Global Health Security Index assesses countries’ health security and capabilities across six categories: prevention, detection and reporting, rapid response, health system, compliance with international norms, and risk environment. Used together with the WHO Joint External Evaluation Tool, the GHX index provides a picture of preparedness for epidemics and pandemics. According to the GHX index, the U.S. and UK rank the first and second in preparedness for pandemics. Sweden, France, and Spain are listed within the top 15. In the Covid-19 pandemic, however, the countries deemed most capable of handling pandemics have recorded a higher-than-average percentage of infection as well as the death rate.
By focusing on the structural features of society, states, and economies, the power of individuals’ choices and short-range responses in determining outcomes tend to be down predicted. One, leadership response specifically concerns the government–the individuals or parties in the position of power – as distinct from regime type. Some political leaders took the outbreak seriously from its emergence and directed the state apparatus to address it. Second, individuals in the public develop risk perception and policy preference from its emergence and form constituencies to push for certain leadership responses. Although individual reactions and leadership decisions are often channeled through institutions, it is clear that they played a significant role in determining governments’ responses in the Covid-19 pandemic.
Risk perception towards Covid-19 at its emergence determined the public behavioral response and swung decision-making in the leadership. The measures that constitute a timely policy response (monitoring, contact tracing, the encouragement of precautionary behaviors, such as hand-hygiene and mask-wearing) are only effective if there is prompt and widespread public compliance. In the total absence of public risk perception, individuals will be driven by a false sense of security and be skeptical about the necessity to implement such measures, up until the moment when the severity of the pandemic becomes evident. Conversely, if a health crisis is perceived as an unknown and unmanageable threat, the public’s response will be driven by fear and lead to socially undesirable behaviors, such as unnecessary stockpiling, scapegoating, and potential stigmatization of minority groups. In order to be effective from a policy perspective, public perceptions of risk should be heightened enough to trigger a reaction in the public, but also moderate enough to lead the public to believe that the threat is manageable and the measures taken can be effective.
Recent experience of similar epidemics raises the alertness towards a potential public health threat while building confidence in the resolution of a public health crisis. At the emergence of the Covid-19 outbreak, the new infectious disease can be understood on a spectrum from seasonal influenza to serious respiratory tract infections that later developed into epidemics like SARS and MERS. However, one often lacks a gradual understanding of the spectrum under time pressure and uncertainties. Instead of perceiving the unknown virus on a spectrum, individuals use a cognitive shortcut by perceiving it as close to one end or another. People with recent experience with SARS and MERS are likely to recognize the risk of such an outbreak turning into an epidemic or pandemic as high but manageable, and people who have only known influenza will recognize the risk either as very low or too high to be contained.
Recognizing the Threat and Sounding the Alarm
In Hong Kong, Macao, Taiwan, South Korea, Singapore, and Thailand, people quickly recognized the threat (i.e. risk of this outbreak turning into an epidemic or pandemic), the governments treated the news with utmost urgency and triggered the maximum level alarm. South Korean media reported that on the next day after the local transmission was confirmed through a church, the streets of Daegu were empty in reaction to the outbreak. A resident described the reaction, stating “it’s like someone dropped a bomb in the middle of the city. It looks like a zombie apocalypse.” National rage rises against government inaction and calls for more proactive measures to contain the spread of the virus. In Hong Kong, it was perceived as a “live-or-die” moment as medical workers strike for comprehensive border control.
From the public to decision-makers, most people in these countries and regions lived through the traumatic experience of SARS in 2003, when the Chinese government’s hiding and manipulation helped the deadly disease spread internationally. Several public opinion surveys in South Korea, Taiwan, and Hong Kong show that the public was constantly worried that governments’ countermeasures were not stringent, comprehensive, and proactive enough. They shared a collective memory of fear about concealed key information and fake death statistics. Experience from SARS largely defined and restricted the understanding about the by-then unknown COVID-19 outbreak, and shaped these governments’ response to control the pandemic. As these governments triggered maximum levels of alarm, standardized reaction protocols were activated. Eventually, their handling of the outbreak based on surveillance and contact tracing proved successful in taming the first waves of imported cases.
Outbreaks of SARS and MERS barely touched the West, potentially leaving the public and leaders too complacent. Furthermore, for most infectious diseases that were once epidemics (like H1N1 and swine flu), many have developed a stoic indifference. Compared to Hong Kong, Macao, Taiwan, South Korea, Singapore, and Thailand, most Western Europe and North American countries initiated surveillance and social distancing much later. Testing, too, was much less rigorous. In countries like Sweden, little attention was paid to the fact that COVID-19 fatalities were highly concentrated among the elderly. As a result, efforts to make community care facilities more equipped to take care of elderly Covid-19 patients were few and far between.
The European Union was first slow in recognizing the threat. EU institutions did not seem alarmed until Italy asked for assistance. Even then, other EU countries were hesitant to acknowledge the severity of the situation. According to a POLITICO article, only on 2nd March the European Centre for Disease Prevention and Control seriously contemplated implications of uncontrolled spread around the bloc for the first time and upgraded the risk to health systems as “moderate to high”. When countries finally recognized Covid-19 as a domestic threat rather than a ‘problem of others’, they decided to take measures to contain it. France started to stockpile personal protective equipment, and Germany published an export ban on such equipment. Across Europe, governments were slow to sound the alarm and still reluctant to disrupt their economies and social life to combat the virus.
In the United States, the administration resisted calls to advise people to stay at home and practice social distancing. Communication was fuzzy, too. Experts have described output from the White House as “a stream of self-congratulatory tweets, mixed messages, and contradictory daily briefings”. Leaders in the West, especially the U.S. President, have focused on the idea that this infectious disease is “foreign”. The metaphors of “foreignness” contribute to false notions of the biological susceptibility to disease in terms of “them” and “us”. In the context of an epidemic, socially and politically meaningful categories can shape discourses of risk, and in turn, political calculations about how to respond. Indeed, President Trump has referred to Covid-19 as “Wuhan disease” and a “Chinese virus”; and has sought to curb immigration in the wake of the epidemic, exacerbating such notions.
Figure 2. Covid-19 Government Response Timeline
The Covid-19 government response timeline marks the time points when national governments took initial countermeasures in response to the Covid-19 outbreak based on the Coronavirus Government Response Tracker. This includes international travel controls (from screening arrivals, quarantine arrivals, ban arrivals to total border closure), public information campaigns, and contact tracing. We can clearly identify three groups of governments: governments of Hong Kong, Macao, Taiwan, South Korea, Singapore, and Thailand adopted proactive and precautionary measures as early as late December; governments of most European and North American countries who implemented early surveillance around late January; and governments of Iran, Brazil, Mexico, and Austria, Switzerland, Denmark, Netherlands and Sweden delayed such measures until late February. Countries that have recently experienced coronavirus epidemics share a more pessimistic risk perception about the Covid-19 outbreak. By recognizing the threat earlier, these governments sounded the alarm sooner. Early warning and early surveillance have proven to be successful in taming imported cases.
Timeliness of Social Isolation
While the decision-making in the first phase of disease control concerns when to sound the alarm and how to control imported cases, in the second phase it should focus on when to implement social distancing measures and how to contain local community transmission. When the virus started to spread locally, governments again faced the difficult decision of whether and when to enforce social distancing policies despite the high economic costs. This includes closing schools and workplaces, cancelling public events, restricting gatherings, closing public transport, restricting internal movement, or public stay-at-home requirements. This choice is a controversial one: if a government acts swiftly and the outbreak isn’t as severe as anticipated, then policy-makers face backlash for overreacting. If one adopts a wait-and-see approach and moves too slowly, then a government might draw criticism for under-reacting.
Timeliness of social isolation is essential in containing local community transmission. In Hong Kong, Macao, Taiwan, South Korea, Singapore, and Thailand, individuals’ sense of urgency was driven in part by recent first-hand experience of how virulent and infectious coronavirus can be due to an outbreak of MERS in 2015 and the 2003 SARS epidemic. Their pessimistic risk perception makes them more tolerant of social and economic costs under isolation. Second, previous governments in these countries and regions had to close schools and cancel public events due to recent epidemics. As a result, current leaders don’t have to deal with the fear of being first-mover, of being the first government in a long while to institute seemingly severe social distancing measures.
On the other hand, although social distancing was proven to be effective in controlling the Asian flu during the 1957–1958 pandemic, that was the last implementation of nation-wide social distancing against epidemics in the UK and U.S. In recent epidemics, social distancing has borne more controversies. During the swine flu outbreak in 2009 in the UK, schools weren’t closed to interrupt the course of the infection, although a group of epidemiologists endorsed it. Outbreaks of SARS and MERS barely touched the West, being contained, like in the case of Ebola, near the site of their outbreak, leaving citizens and leaders complacent and unprepared. Indeed, when it came to implementing social isolation in order to contain Covid-19, many governments in Western Europe found it extremely challenging. Multiple factors may have delayed their decision-making, including the careful balancing between mitigating public health risks and paying economic costs, contrasting scientific evidence, and potential fatigue problems.
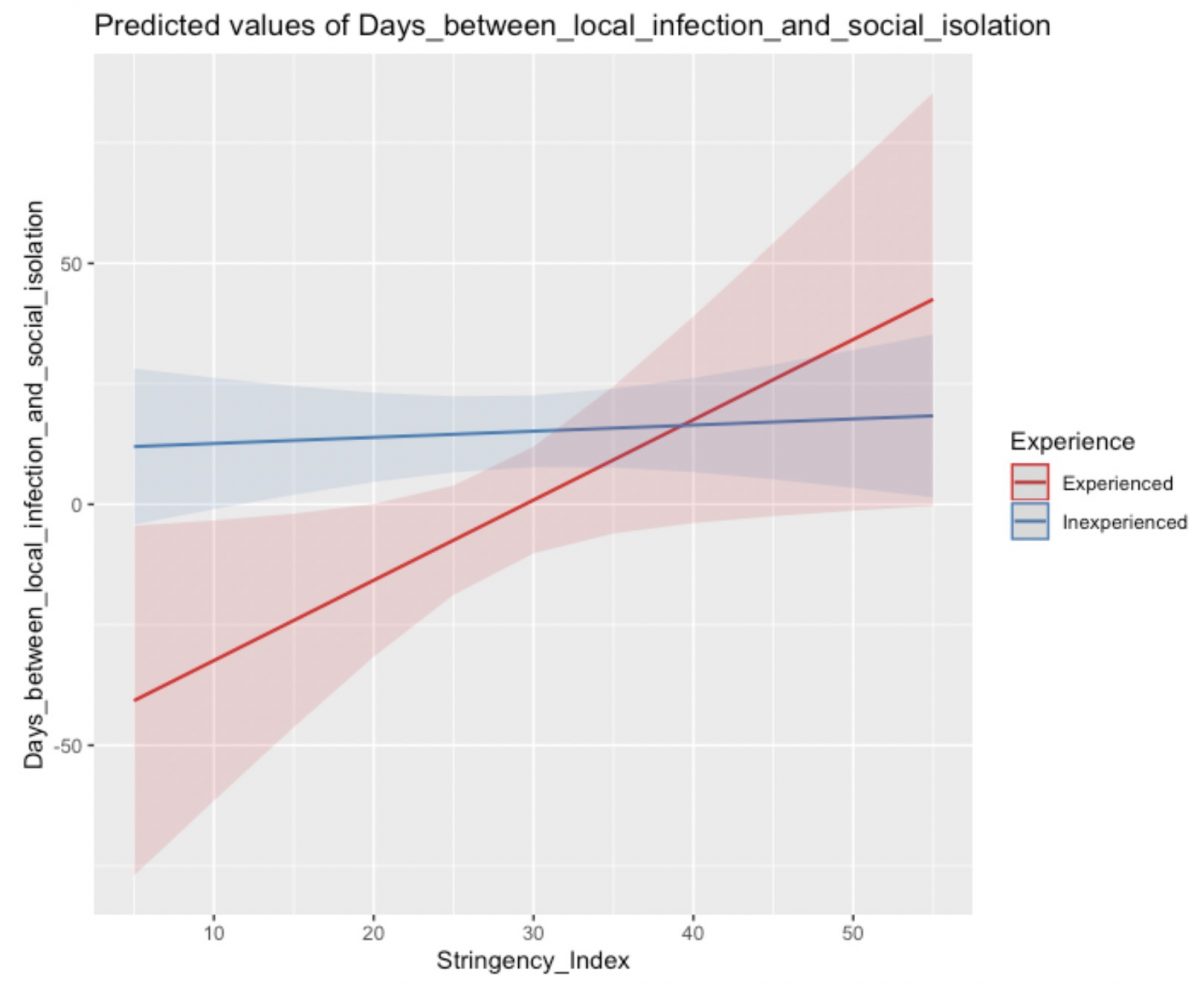
To measure the timeliness of social isolation for individual countries, we count the number of days between the first possible local cluster transmission and first social distancing policy. On average, governments took 11 days to introduce social distancing after local community transmission was detected. As we predicted, governments experienced in enforcing social distancing measures before – including Hong Kong, Macao, Taiwan, South Korea, Saudi Arabia, and Mexico (Mexico experienced swine flu in 2009) – decided to introduce social isolation faster than the global average. On the other hand, the U.S. (44 days), UK (50 days), India (34 days), Spain (37 days) and France (38 days) took significantly longer to make such a decision. Further examination on the systematic difference between social isolation responses show that governments with recent experience in epidemics introduce social distancing policies significantly earlier than their counterparts in the Covid-19 outbreak (see figure 3).
When lockdown is delayed, experienced governments step up more decisively in their testing and tracing efforts, thus reducing the need to implement strict social isolation. Such was the case of Singapore. Although multiple local clusters were identified as early as 4 February, there were only around a hundred infected cases and no deaths until late March. As a result, social isolation was only introduced 38 days after the first local transmission, but with more stringent measures, more comprehensive coverage, and much stricter enforcement.
Figure 3. The difference in timeliness between countries with and without recent epidemic experience
Conclusion
The Covid-19 pandemic has left an indelible mark on our societies and on our perceptions of politics and institutions. Even though we don’t seem to be close to the end of the tunnel, there are some important lessons that should be learned by considering the role that previous experience played in shaping a country’s performance during the current pandemic. This pandemic is a humbling experience, since previous exposure to viral epidemics is not something determined by human will and good political choices, but by chance. And, despite the sorrow that the current health emergency has brought all around the world, it also gives reasons for hope. Covid-19 has reached people all over the globe, both in rich, Western countries and in the global South. It has entered our collective memory and shaped the way that we will likely perceive future public health risks. The Covid-19 pandemic is a positive shock to the system, based on which governments can seek to improve both long-range investments in preparedness and short-range response to future outbreaks.
This crisis constitutes additional evidence to the idea that even though policy learning and assessment are the often-neglected steps in the policy-making process, they are the ones that bring about most of the progress. It is hard to gather the will to objectively evaluate a policy after all the effort that has been put in its development and implementation. However, it is also the crucial step to understand whether an issue has been adequately addressed, whether incremental adjustments should be made or if the policy should be discarded altogether. Both SARS and Covid-19 caught the respective governments unprepared, and the immediate political costs of policy learning were high. However, as seen in places like Taiwan and Hong Kong, the long-term benefits of honest and comprehensive policy evaluation largely overcome its costs.
Further Reading on E-International Relations
- Global Health Diplomacy and the Security of Nations Beyond COVID-19
- Can Populism Survive COVID-19?
- Africa’s Disproportionate COVID-19 Pandemic
- Opinion – Nationalism and Trump’s Response to Covid-19
- The International Political Economy of Health: The Covid-19 Vaccine Distribution
- Opinion – How to Call the COVID-19 Pandemic and Why it Matters