
As the COVID-19 pandemic spread from one region to the next, an interesting picture began to emerge. As researchers pointed out, there seemed to be an anomaly occurring on the African continent. Early warnings of the viral tsunami about to hit all regions of the populated world included dire forecasts for the African continent. Plagued with poverty, general underdevelopment, poor infrastructure, corruption, and under financed and poorly maintained healthcare systems, the evolving picture for the continent was critical. But, Africa’s place in the global crisis developed as an unexpected and counterintuitive one. As one of the poorest and most underdeveloped regions of the world, Africa seemed to be defying those expectations with low numbers of COVID-19 cases and low numbers of deaths.
As Figure 1 shows, as , the World Health Organization declared a Public Health Emergency of International Concern on January 30, 2020, Africa’s COVID-19 cases were non-existent in the reported data, though this did not mean that there were no cases.
Figure 1. Number of Cases and Case Deaths in Africa as of June 11, 2020. Data Sources: Max Roser, Hannah Ritchie, Esteban Ortiz-Ospina and Joe Hasell. 2020. “Coronavirus Pandemic (COVID-19)”. Published online at OurWorldInData.org; European Centre for Disease Prevention and Control (ECDC). 2020. “COVID-19”.
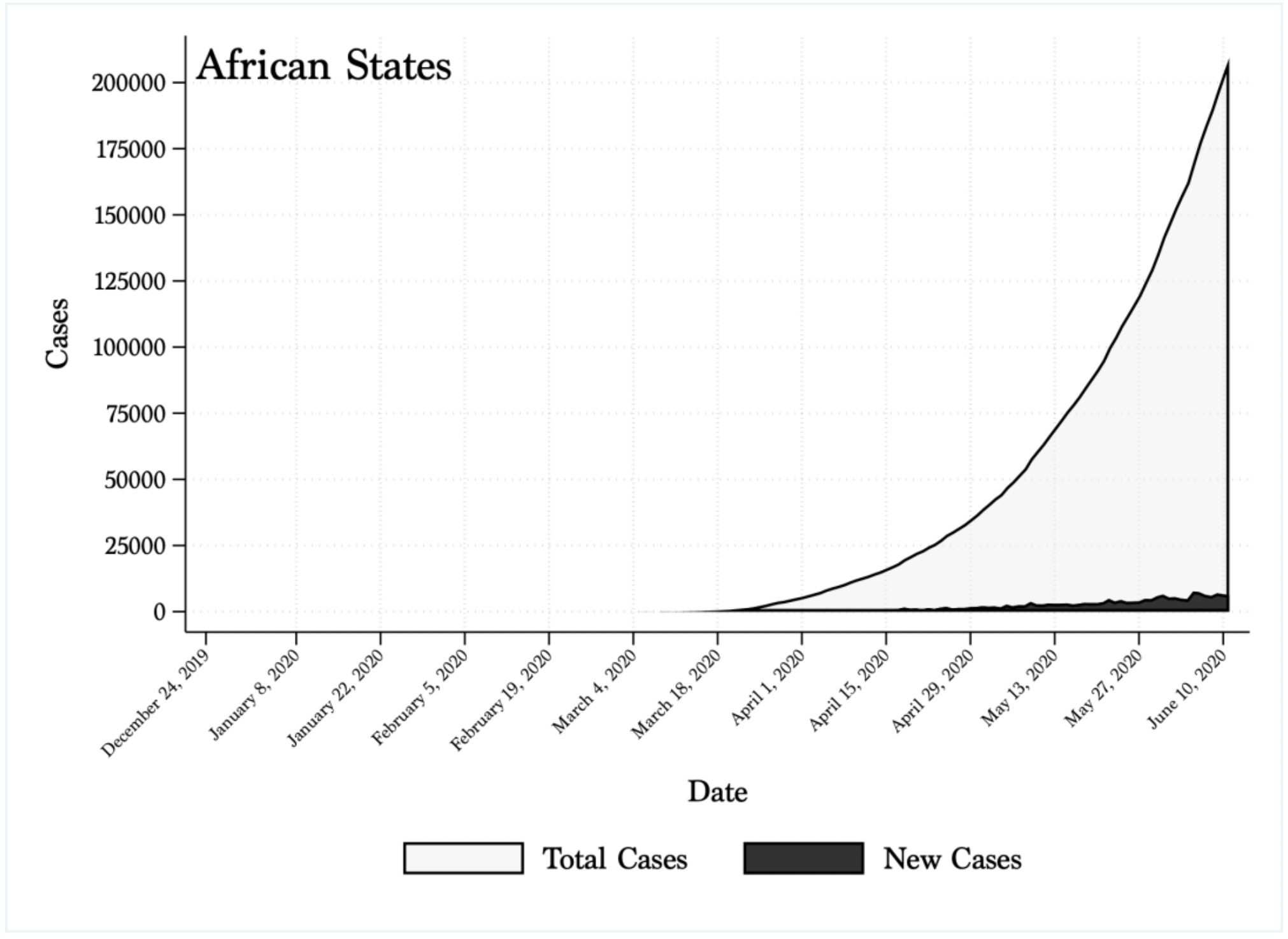
Similarly many countries, developed and underdeveloped, the lack of testing and data collection meant the true picture of the pandemic’s extent was, and currently still is, unknown and may never be known. As the pandemic spread, Africa’s numbers through April remained relatively low compared to other regions. But, in recent weeks, the total number of cases has risen by almost 45 percent across the continent.
Analysts and public health officials attributed the initial situation on the continent to a host of factors: Africa’s large youth population (70% of people under the age of 30), policies enacted by governments, Africa’s prior experience with epidemics such as HIV, Yellow Fever, Cholera, and Ebola, and even the continent’s heat and humidity levels. Each of these ideas has a basis of truth. But all have an underlying problem, which is that they engage Africa as a homogeneous entity, with no nuance or sense of the political and socio-economic dynamics at work on the continent. Like many regions of the world, Africa is one of significant variation.
Africa’s Big Eight
When Africa’s relatively quiet navigation through the COVID-19 pandemic came to an end, the news reflected this homogeneous view of a continent now on the brink of viral catastrophe. While every country on the continent now has COVID-19 infections, the data indicate that a large portion of the continent’s cases are being driven by eight countries out of 54 across the continent: Algeria, Egypt, Ghana, Morocco, Nigeria, South Africa, Cameroon, and Sudan. As Table 1 shows, the proportion of cases and deaths these countries account for is substantial.
Table 1. Cases and Deaths of the Top Eight African COVID-19 Infected Countries as of June 11, 2020. Data Sources: Max Roser, Hannah Ritchie, Esteban Ortiz-Ospina and Joe Hasell. 2020. “Coronavirus Pandemic (COVID-19)”. Published online at OurWorldInData.org; European Centre for Disease Prevention and Control (ECDC). 2020. “COVID-19”.
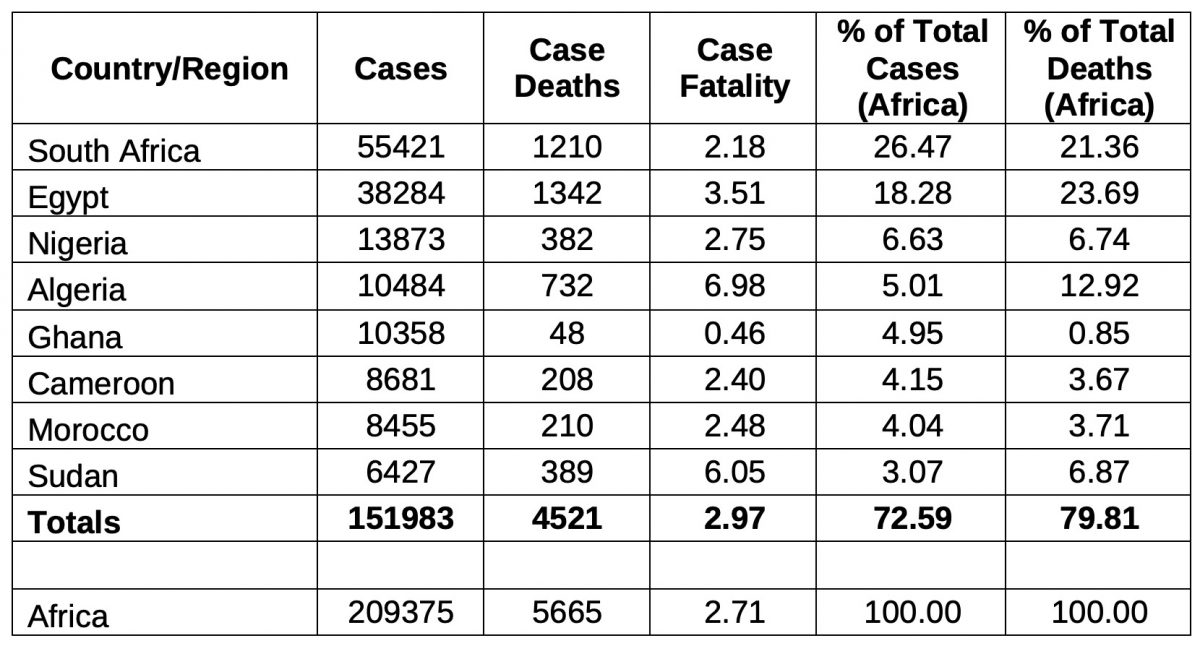
While the number of cases is a relatively meaningless number in terms of what is actually happening with the pandemic, it does provide a snapshot of a situation that is changing daily. Collectively, these eight countries account for 72.6 percent of the cases and almost 80 percent of the deaths on the continent. The fatality rates across the eight countries range from .46 (Ghana) percent to almost 7 percent (Algeria), with Africa’s fatality rate being about 2.7 percent. The rest of the countries on the continent account for less than 28 percent of the infections. This pattern is not unique. In South America, for example, while the numbers are larger, the pandemic has been driven largely by three countries: Brazil (61 percent of cases), Chile (12 percent), and Peru (16 percent), while other states are showing signs of increasing viral stress.
Each of the eight countries have experienced an uptick in cases heading into the April-June period. While Ghana has a low number of deaths, a number of the countries are seeing an uptick in the number of deaths in conjunction with the increase in cases. The numbers are still relatively small compared to other countries and regions, but Algeria, Egypt, Nigeria, and Sudan have shown more recent increases in the number of deaths associated with the pandemic. In light of the recent large increase in the reported cases, public health experts have warned that the worst may yet be coming for the continent. Additional figures showing case and death data for Algeria, Cameroon, Egypt, Ghana, Morocco, Nigeria, South Africa and Sudan can be downloaded here (PDF).
The countries driving the COVID-19 pandemic in Africa are microcosms of the continent itself – ethnically, economically, politically, and socially diverse. Thus, it is difficult to pinpoint these types of macro-level indicators as influential factors in pandemic, much like it is difficult to pinpoint these same factors in other countries and regions. It is possible that they act as undercurrents, but these are variables that are idiosyncratic. Regardless of the macro-level explanations, the factors that have influenced and mitigated this and other epidemic and pandemic spreads are not idiosyncratic: the role of leadership and messaging and the adherence to socially based practices.
Leaders, Leadership, and Those that Don’t Follow
Leadership plays an important role in the direction that pandemics and epidemics take, and it serves several functions. In any crisis, political leaders are the decisionmakers providing direction for a plan to resolve it. Technical experts recommend operational plans to respond to outbreaks, but political leaders direct the plan. Leadership also involves shepherding people and resources to combat problems. In pandemics, strong political leadership unites the population behind one message and plan: stop the virus.
Federal political leadership makes the decisions about how to prioritize issues, to expend increasingly scarce resources, and to whom those scarce resources go. Local leadership is the driving force to enact those policies and priorities. Transparency in these policies and priorities minimizes public panic and promotes coordination among federal governments, subnational states, local leaders and health advisors and policymakers. But transparency from political leaders and public trust in those leaders are in short supply on the continent, as it is in many other regions of the world. One phenomenon common to most African states is a long history of post-colonial strong-man leaders that have often left their states institutionally weak, corrupt, and vulnerable to economic, social, and political strife. Such rulers have left state-societal relationships weak and with citizens suspicious and cynical of leaders at any level of government. Data bare out this problem.
Table 2 presents data from the latest 2016/2018 cohort of Afro barometer surveys for six of the eight most afflicted countries. Algeria and Egypt were not available but previous studies in the series support the following conclusions. While the data are a bit older than the current crisis, people’s trust in leadership is not a rapidly changing facet of opinion. The data are consistent across all six countries and consistent in previous years.
Table 2. People’s Perceptions of Trust in Leaders, 2016/2018 Cohort. Source: Afrobarometer, 2016/2018 State Cohort.
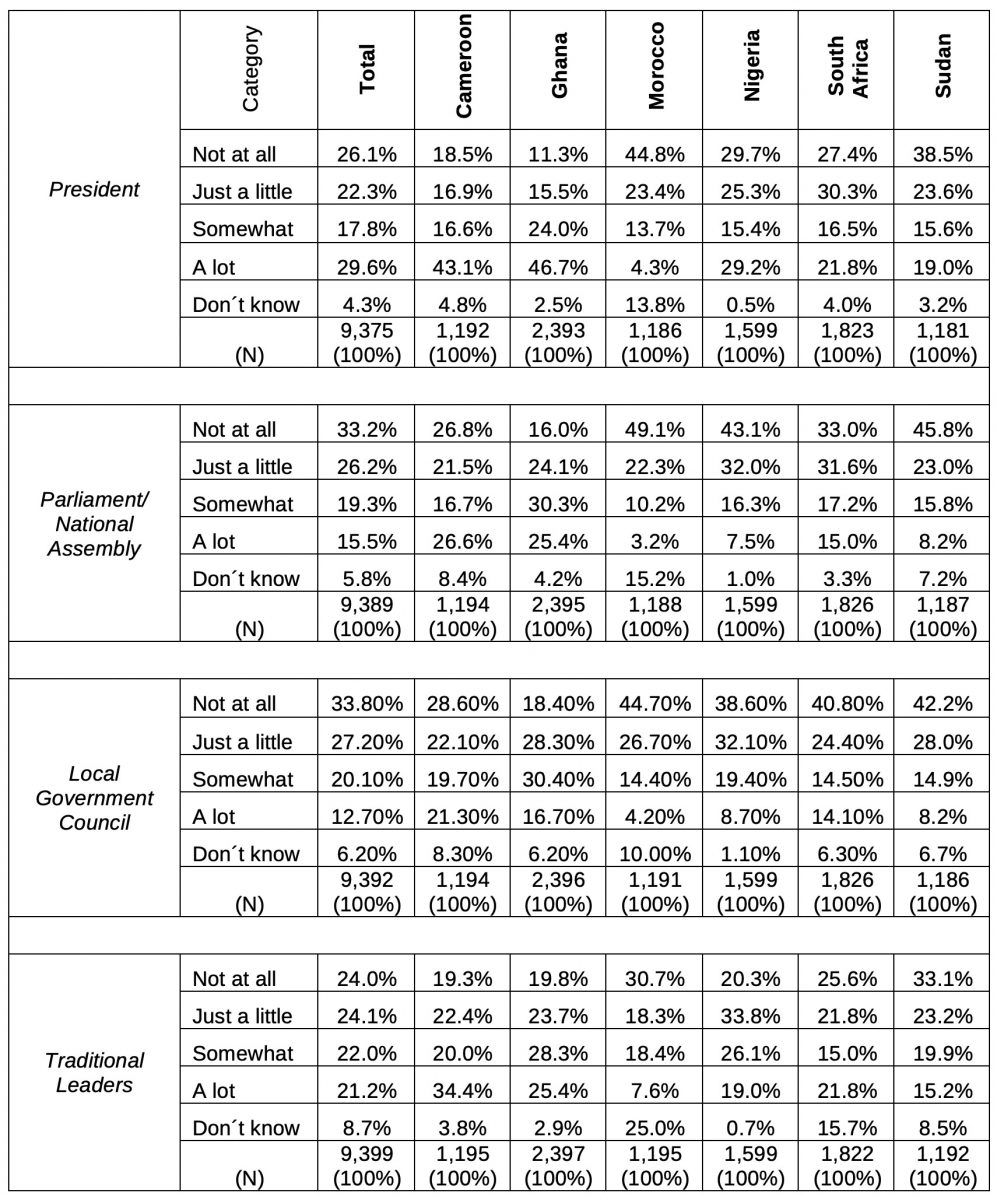
At no level of leadership, in no country do people trust their leaders “a lot;” in some countries that number struggles to break 10 percent of those surveyed. Some of the data may represent a healthy skepticism of political leaders (“somewhat”) but the data are clear in that the majority of those surveyed have little to no trust in their leaders from the national level (president and national legislatures) to the local and personal level (local councils and traditional leaders). Thus, when leaders enact policies to deal with a disaster such as a pandemic or epidemic, one can easily conclude that people question the necessity, motives, and objectives of those policies.
In responding to the COVID-19 pandemic, the eight African states have generally enacted national or subnational level policies, above the local level, that address key factors that public health officials have identified as ways to mitigate the spread of the pandemic. While it is difficult at this moment to gauge how effective each of these policy areas has been, they can indicate whether state leaders are addressing important policy factors and whether they are enforcing those policies or people are following them. Table 3 highlights a series of policy pronouncements and statements that states have addressed at municipal, provincial/state, and national levels.
The data indicate that the eight African states have addressed key points across 17 specific policies related to state responses to the COVID pandemic; however anecdotal evidence suggests the policies have been enacted unevenly and, in some cases, with little conviction or enforcement, and in other cases stringent and harsh enforcement. While the data are most likely incomplete, particularly at the local/municipal level, they do present patterns that show how states have reacted to the pandemic.
While some leaders, such as South African President Cyril Ramaphosa, have received praise for acting quickly in the early stages of the pandemic, even their performances have sent mixed signals to the public about the severity of the pandemic in their countries. So, while Ramaphosa enacted and enforced a series of stringent policies, his flaunting of these policies in public, not wearing a mask, ignoring social distancing, and joking about the policies, sent mixed signals about how seriously others should take the pandemic. Other countries have experienced the same type of issues with leaders and with affected people.
Algeria and Sudan have been the least responsive overall from a policy perspective. During the pandemic, Algeria’s political leadership has focused on tightening its grip over Algerian society in the wake of the popular uprising that overthrew President Abdelaziz Bouteflika. Similarly, Sudan’s junta, in the wake of the popular revolt and coup that ousted its long-standing dictator Omar al-Bashir last year, has been generally absent from and even flaunting COVID-related policies that could mitigate the virus’s spread. While Egypt has responded to the pandemic more so than Algeria and Sudan, its transparency in doing so has been questioned, leading to suspicion and distrust.
Table 3. Policy Areas Addressed in the COVID-19 Response. Source: Cheng, Cindy, Joan Barceló, Allison Hartnett, Robert Kubinec, and Luca Messerschmidt. 2020. COVID-19 Government Response Event Dataset (CoronaNet v1.0).
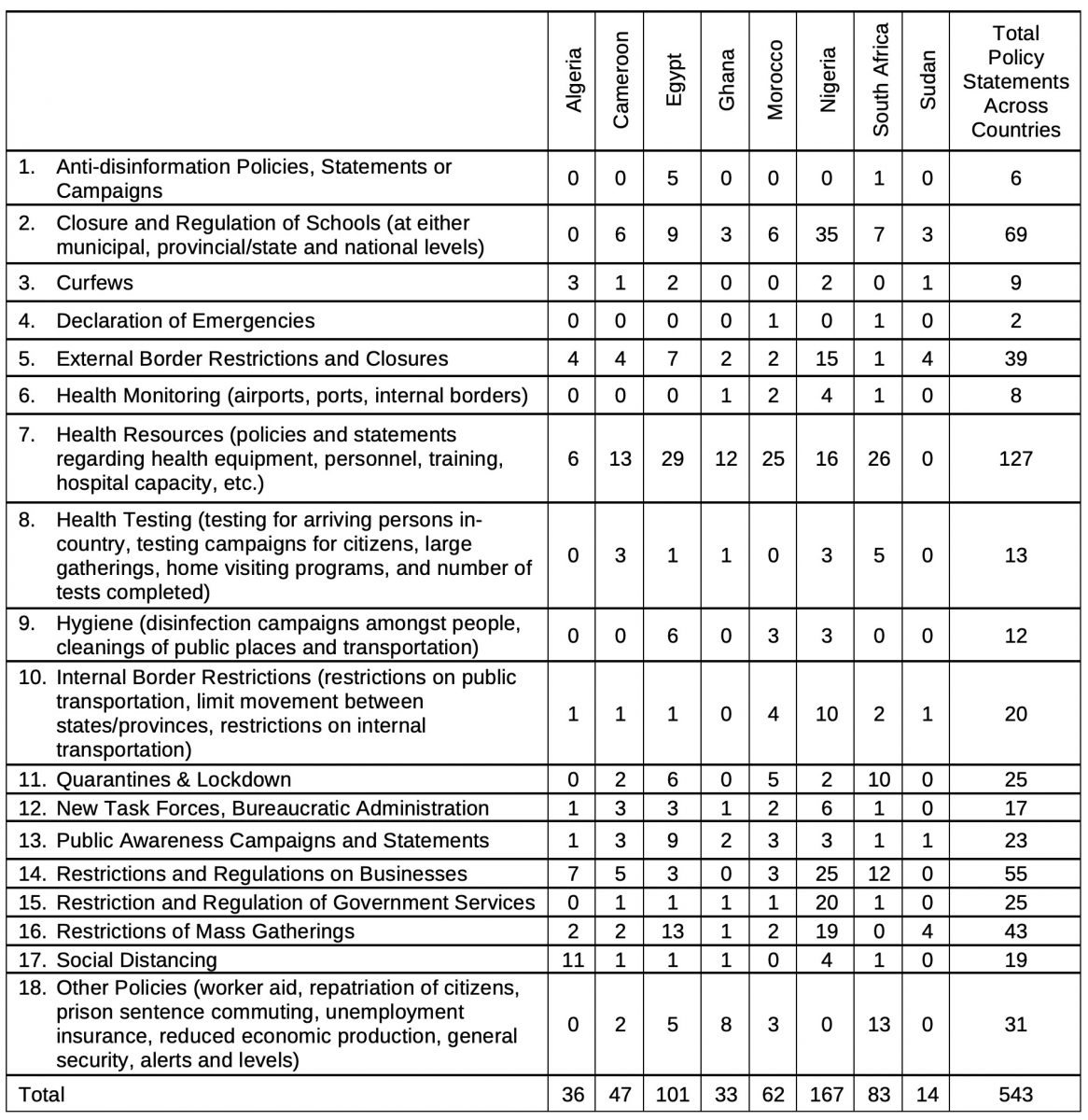
Egypt, South Africa, and Nigeria, the hardest hit African countries in the pandemic, have been the most policy active states, though there is some interesting variation. Egypt has a strong central government and 92 percent of the policies released have been by the central government. In comparison, Nigeria which has a weaker central government in a federalist system, has had 83 percent of its policies and statements made at the provincial/state level, and South Africa in a contested federalist system, has had just three percent of its policies stated or enacted by provincial and state governments. Ghana, Sudan, Cameroon, Morocco, and Algeria also have had the majority of their policies stated or enacted by the national government.
In the 1918 Spanish influenza pandemic, uncoordinated state-level responses in the United States helped to spread the virus into new areas of the country. Certainly, national, provincial and state level policies that are mostly uncoordinated across different levels of government may be contributory factors that have failed to mitigate the spread of the virus. For most of these eight countries, one problem appears to lie with the impression that political leaders have ignored how policies are to be carried out and what resources are needed to do so.
The policies themselves also indicate some variations and patterns though the pictures are incomplete. The fewest policies issued were relative to declarations of emergencies, anti-disinformation campaigns, health monitoring, curfews, hygiene, health testing, new task forces, social distancing, and internal border restrictions. These policies represent difficult policies to implement and to enforce within each country.
For instance, controlling rumors and social media in some countries is difficult in non-pandemic conditions; however, disinformation potentially causes panic and can build anti-government or anti-opposition sentiments that feed people’s suspicions and lack of trust. Hygiene, health testing, social distancing, new task forces, and internal border restrictions are resource-intensive and difficult to enforce without commitment of resources that many governments may not have or may not be willing to expend. But, at the same time, these are also policies needed to control the pandemic.
Testing, social distancing, hygiene, and movement restrictions play important roles in curtailing viral spread. Other policy areas such as quarantines, restricting government services, external border restrictions, and closing schools and businesses are easier to employ with resources that are mostly deployed already (bureaucracies, police, military, and other security personnel).
The largest segment of the policy pronouncements concern health resources. Given the nature of the crisis, this makes sense. Close to a quarter of the policies and statements issued by the governments were related to the resources needed to battle the pandemic. Interestingly, of the 127 policy statements and pronouncements issued across the eight countries, national governments made almost 80 percent of those statements and policies. Thus, the national governments have at least said what they should be in this regard – marshalling resources particularly given the limited resources available to provincial and state level governments.
As many regions have shown, the lack of resources can be devastating. For instance, the lack of hospital space and other medical facilities have led Algerians to refer to hospitals as “places for dying,” as hospitals struggle to maintain pace with the spread of the pandemic. While some resources are needed to be effective, particularly in the area of health resources, not all policies are financially expensive; sometimes they are behaviorally intensive. The currency that states need to implement those policies is trust and transparency, often in short supply in many countries across the globe.
African states have already come under scrutiny for the way in which they are enforcing pandemic policies. All eight of the most afflicted African states have been accused of violating or potentially violating the rights of their citizens; international and civil society groups have accused Ghana Egypt, Cameroon, Algeria, South Africa and Morocco, Sudan of policies ranging from bypassing government oversight of COVID-19 policies to measures of harsh repression.
While African states have shown mixed results in responding to the pandemic, the citizens have presented problems in following recommended guidelines; those problems range from basic economic issues to deeply entrenched cultural practices. Policies directed toward social behavior, lockdowns, quarantines, social distancing and others, have significant impacts on people’s livelihoods in all countries, giving incentive not to comply.
Impoverished people in secondary labor markets are most at risk as their livelihoods are often linked to service sectors that are severely affected by pandemic policies. In Sudan, protests have emerged as people see the COVID-19 pandemic as a choice between death by virus or death by starvation. The same problem is present in Morocco as well. Food security is not a problem unique to the African continent, as the World Bank has noted.
In Ghana, people still attend elaborate memorial services for the dead, causing a backlog at morgues while providing more opportunity for exposure to the virus in large gatherings. In Sudan, a lack of information and the belief that the pandemic would not arrive gave people reason to ignore social distancing and mass gathering policies. Local newspapers have shut down and only about 26 percent of people have access to news disseminated through the internet. There has been no local enforcement of policies such as curfews and bans on gatherings.
In Cameroon, hospital workers have been attacked by people in denial concerning positive COVID-19 tests for them or their relatives. People have even exhumed covid-19 victims to give them a “…proper burial.” While masks are required in Cameroon, some cannot afford them and many go without them.
In Nigeria’s northern city of Kano (population 5 million people), doctors and nurses are so infected with the virus that hospitals are not accepting patients. There is little to no social distancing or masks worn, and grave diggers are working overtime. In Lagos, Nigeria’s economic hub with a population of 20 million, social distancing and other protection policies are openly ignored. As one person in Kano said, “The leadership is in denial.” To make matters even worse, doctors across Nigeria went on strike (called off as of June 21) over wage disputes. Despite the hotspots in Nigeria, religious leaders are demanding that restrictions on religious gatherings be abandoned.
Similarly, in Egypt, the virus has overwhelmed hospitals with cases, making it difficult for people to find treatment. People and medical officials have accused the government of negligence in its response, but have also often ignored basic pandemic social policies to help curtail the virus’ advancement. Social distancing is difficult, if not impossible, to enforce in some of Egypt’s crowded cities.
In South Africa’s impoverished black townships, close confines and neighborhood cultures have been reason for people to ignore bans on mass gatherings and policies on social distancing. Military and police patrol densely populated townships trying to enforce pandemic policies; that effort has had mixed success with human rights violations occurring in the process of enforcement.
When the situation in Africa is examined closely, the numbers tell a story of an increasingly dangerous pandemic that political leaders have responded to in mixed fashion and the people have responded to with either the inability to follow public health directives or an unwillingness to do so. In other words, African states, with varying specific details, are just like other states and regions of the world confronting a pandemic that is spiraling out of control. It may be the case that African states may face an increasing threat from the pandemic. It may be the case that African states are vulnerable because of their political and developmental problems. But it is not the case that these problems are unique to African states or that the entire continent will necessarily feel the brunt of the pandemic.
At the political level, problems in political leadership stymie effective responses; at the social level, the inability or unwillingness to follow public health recommendations prolong the hard political and economic hardships brought on by the new reality of living in a pandemic. Both are failures of leadership that may have catastrophic consequences. How the pandemic unfolds on the continent will be a manifestation of how the political leadership reacts and how the people respond, problems no different than in the epicenters: the United States and Brazil, and other areas currently in the midst of the pandemic.
To be certain, African states have a myriad of problems that they have had to confront well before the pandemic hit them. Their smaller connections to each other and to the rest of the world may have slowed the pandemic’s advancement on the continent. But it is clear that the virus is now hitting African states head-on, but disproportionately. Some of their problems will make coming out the other side of the pandemic more difficult than other states in the international system may experience. Poor health infrastructure, discredited leaders, endemic poverty, and other socio-economic constraints make any crisis complicated for African states. In the current pandemic, co-morbidities such as HIV/AIDS, tuberculosis, cholera, and malaria also may complicate the COVID-19 situation in many states.
Despite these issues, African states’ challenges in confronting the pandemic are not all unique to them. Disinterested and misinformed leaders, societal distrust in leadership, and political and social dynamics complicate the implementation of coordinated policies to push back the pandemic no just on the African continent, but also in European, Latin American, Asian, and North American states. In this sense, African states and their people provide lessons to learn about pandemic responses, both positive and negative.